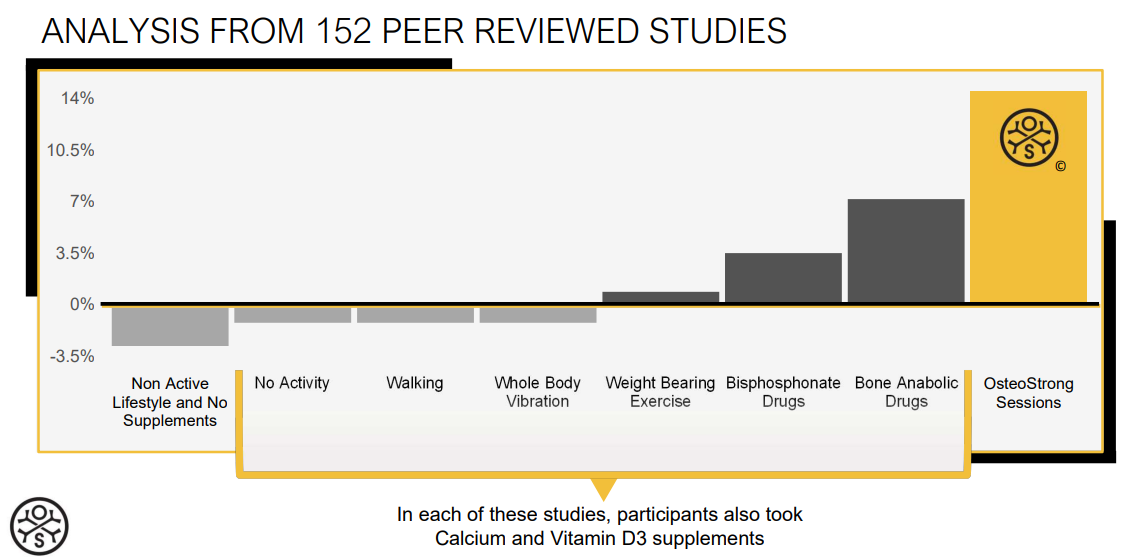
Non active lifestyle, no supplements
- In 2003, the New England Journal of Medicine published an article that established that after the onset of menopause, females may lose 1.9% of their bone mass density per year(3).
No activity w/ Calcium and vitamin D, abbreviated: (C&vD)
A compiled analysis of 29, all randomized trials found supplementation with calcium and vitamin D was able to slow bone density loss between the hip and spine over the course of a year by half of the standard amount of loss given the other variables in an individual’s life(4).
Walking + vitamin C&D
- A compiled analysis of 8 studies found brisk walking type exercise showed no bone density gain between the hip and spine over the course of a year(5).
Whole Body Vibration + vitamin C&D
- A compiled analysis of 18 studies found whole body vibration (WBV) showed no bone density gain between the hip and spine over the course of a year, but positive implications were seen with activation of muscle, and help with balance and proper movement(6).
Weight Bearing Exercise + vitamin C&D
- A compiled analysis of 62 studies found weight bearing exercise showed an average of 1% bone density gain between the hip and spine over the course of a year(7).
Bisphosphonate Drugs + vitamin C&D
- Bisphosphonate drugs like Boniva, Actonel and Fosamax which are the standard of care can show an average of 1.6% bone density gain between the hip and spine. Learn more by discussing these drugs with your physician(8).
Bone Anabolic Drugs + vitamin C&D
- Forteo is a bone anabolic, which has shown an average of 6.15% bone density gain between the hip and spine. Side effects can potentially include increased cancer risk for those who have risk factors. As this drug is newer, much is still to be learned. This drug is only prescribed for patients at high risk of fracture, and patients have to be monitored closely for adverse effects. Learn more by discussing these drugs with your physician(9,10).
Osteogenic Loading
- The use of osteogenic devices like the ones used at OsteoStrong have shown promising results. Though there are only 4 studies on the specific application of osteogenic loading devices, the underlying principle is one of the most fundamental of human physiology (mechanotransduction) and as loads seen with osteogenic use are far beyond the minimum established trigger for building bone, the results seen are beyond that of other treatments. Bone density has been shown to improve 7.34% between the spine and hip results over one year of treatment(11). Further, Hunte and researchers found bone density gains of over 14% in 6 months of treatment(12). Further research shows statistical congruency with a larger sample (n=2300) for functional bone performance gains and BMD(13).
Osteogenic loading is not for everyone. People with un-medicated hypertension, muscular dystrophy, or the lack of proper pain-free movement to perform the osteogenic loading protocol should consider other options. However this being said, as there are no adverse effects most can try it first, and learn about how it works for them without compromising their health.
Sources:
- Forwood, M. & Burr, D. (1993). Physical activity and bone mass: exercises in futility? Journal of Bone and Mineral Research. May;21(2):89-112.
- Tobias, J. H., Gould, V., Brunton, L., Deere, K., Rittweger, J., Lipperts, M., & Grimm, B. (2014). Physical activity and bone: may the force be with you. Frontiers in endocrinology, 5.
- Ahlborg, H. G., Johnell, O., Turner, C. H., Rannevik, G., & Karlsson, M. K. (2003). Bone loss and bone size after menopause. New England Journal of Medicine, 349(4), 327-334.
- Tang, B. M., Eslick, G. D., Nowson, C., Smith, C., & Bensoussan, A. (2007). Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis. The Lancet, 370(9588), 657-666.
- Lau, R. W., Liao, L. R., Yu, F., Teo, T., Chung, R. C., & Pang, M. Y. (2011). The effects of whole body vibration therapy on bone mineral density and leg muscle strength in older adults: a systematic review and meta-analysis. Clinical rehabilitation, 25(11), 975-988.
- Martyn-St James, M., & Carroll, S. (2008). Meta-analysis of walking for preservation of bone mineral density in postmenopausal women. Bone, 43(3), 521-531.
- Wolff, I., Van Croonenborg, J. J., Kemper, H. C. G., Kostense, P. J., & Twisk, J. W. R. (1999). The effect of exercise training programs on bone mass: a meta-analysis of published controlled trials in pre-and postmenopausal women. Osteoporosis international, 9(1), 1-12.
- BONIVA® (ibandronate sodium) INJECTION. (2011). Retrieved from http:// www.accessdata.fda.gov(Reference ID: 2895743)
- FORTEO® teriparatide (rDNA origin) injection 750 mcg/3 mL. (2008). Retrieved from http://www.accessdata.fda.gov(Reference ID: PA 9244FSAMP)
- Berg, C., Neumeyer, K., & Kirkpatrick, P. (2003). Teriparatide. Nature reviews Drug discovery, 2(4), 257-258.
- Jaquish, J. (2013). Multiple-of-bodyweight axial bone loading using novel exercise intervention with and without bisphosphonate use for osteogenic adaptation. Osteoporosis International. 198; 24(4), s594-s595.
- Hunte, B., Jaquish, J., & Huck, C. (2015). Axial Bone Osteogenic Loading-Type Resistance Therapy Showing BMD and Functional Bone Performance Musculoskeletal Adaptation Over 24 Weeks with Postmenopausal Female Subjects. Journal of Osteoporosis & Physical Activity, 3(146), 2.
- Huck, C. & Jaquish, J. (2015). Functional bone performance measurements and adaptations using novel self-applied bone loading exercise apparatus. Osteoporosis International. 26(1),s391-s392,NS12.